

Protect Trans Kids

Why are people such assholes to trans minors?
Recently, the UK’s High Court ruled that minors can only be given puberty blockers with the permission of a court. It came to this conclusion because 1) puberty blockers are just too experimental (they aren’t), and 2) most people on puberty blockers go on to take cross-sex hormones. (See paragraphs 64, 68, 134, 137, 151, and 152 in the ruling (PDF).) This second point is genuinely idiotic. Apparently, the High Court would be happier if a substantial portion of people given puberty blockers apparently didn’t need it. This is such an ass-backwards reasoning that it strains belief.
The United States is seeing its own version of this hysteria. This past year has seen a blitz of conservative lawmakers trying to overrule medical consensus in an attempt to protect children from the Republican’s own paranoid delusions. To make matters even worse, much of this push is artificial; it is an attempt to create a wedge issue, not something stemming from anything resembling ethics.
I do not normally write with such strong emotional language. In this case, I believe it is quite justified. The sheer level of blatant misinformation being taken as fact, combined with the plainly obvious harm it causes, is infuriating. I do not expect people to spend their time reading studies or leisurely perusing standards of care like I do. I do expect people to have the shred of sense necessary to smell the blatant BS. A sudden, concerted, and partisan effort to get people to believe that the transgenders are ruining children, directly after dropping all the bathroom laws and, prior to that, attacks on marriage equality, is something that anyone should be able to recognize as a cynical ploy.
So, let’s talk about transgender children. And let’s do it right. Start with the professionals and the science. We will not be starting with books written by people outside the relevant fields or websites promoting hearsay, Reddit links, and shoddy biology. To the best of my ability, I will show my work. Feel free to check it.

What is written below aims to be a fairly comprehensive overview of the contemporary standards of treatment for transgender youth, including the risks involved and points of controversy and ambiguity. If you heard something like “puberty blockers make children’s pinky toes explode!” and you don’t see it mentioned below, it is nearly certainly not true.
Transgender kids
Let’s first dispense of some the myths surrounding how trans and other gender-nonconforming (TGNC) kids are treated. TGNC adolescents will be discussed in a moment. There are two, and only two, main schools of thought. Anything else is heterodox and espoused only by a small minority of clinical professionals, and therefore ought to be treated with a strong dose of skepticism. Attempts to encourage children to be cisgender are outside the bounds of good practice, and are considered unethical by every major group which has spoken on the issue. (This account of the two main schools of thought draws heavily from Ristori & Steensma 2016, “Gender dysphoria in childhood”.)
The first approach is sometimes called “watchful waiting.” The mindset of this approach is that there is a very real chance that the gender dysphoria will dissipate as the child ages, so it is important to balance alleviating gender dysphoria now with keeping future options open. For example, while social transitioning (wearing different clothes, going by a different name) can be undone, that doesn’t mean it’s easy to do so. So, keeping in mind the fact that it’s possible the storm just needs to be weathered for a few years, such actions should carefully considered so as to not cause unnecessary trouble down the line. Since the emphasis is on keeping possibilities open, a space must be maintained for the child to explore their gender.
The second approach is focused on positively affirming the child’s own sense of gender and encouraging the development of resiliency and positive self-identity. The child is supported in their gender identity and/or expression. Therapists help the child work through their feelings and navigate social problems, while their guardians support their child’s attempts to explore and express their gender.
Neither approach supports medical interventions, and both approaches have support from intelligent, educated, and ethical professionals. My understanding is that the debate between these two approaches is made murkier by the conflation of children with gender dysphoria proper and gender-nonconforming children. Many of the studies which purport to show a high rate of dysphoric children desisting group together those with gender dysphoria proper and those who are “sub-threshold” and therefore don’t meet the requirements for a gender dysphoria diagnosis. My best understanding is that the former approach is justified when dealing with a child who does not meet a gender dysphoria diagnosis, while the latter is justified for those children who do, and especially those which are consistently, insistently, and persistently dysphoric.
Transgender adolescents

Puberty blockers
Notice that, above, there is no support for medical interventions. That is because there are no medical interventions done prior to puberty. That question only becomes relevant when discussing adolescents.
Adolescents with gender dysphoria are much more likely to identify as transgender as an adult than children with gender dysphoria (Nealy, 2019, p. 22; Coleman et al., 2012, p. 11). Once puberty has begun, the standard approach is to give them puberty blockers — basically, pressing the pause button on puberty. Puberty blockers are regarded as entirely reversible, since once you stop taking them, puberty simply resumes. Puberty blockers are supported as an option by basically every group worth caring about: The World Professional Association for Transgender Health (WPATH) (PDF), the Endocrine Society, and the American Academy of Pediatrics, for example. (Much of this essay draws on these three sources.) The level of emphasis put on puberty blockers varies. For example, the WPATH Standards of Care (SoC) v7 descriptively notes that puberty blockers aren’t available everywhere and the requirements for receiving puberty blockers can vary from clinic to clinic. The Endocrine Society suggests “that adolescents who meet diagnostic criteria for GD/gender incongruence, fulfill criteria for treatment, and are requesting treatment should initially undergo treatment to suppress pubertal development… [and] that clinicians begin pubertal hormone suppression after girls and boys first exhibit physical changes of puberty,” (statements 2.1 and 2.2 under the Endocrine Society link above) while the American Academy of Pediatrics simply notes that puberty blockers are likely to help.
While we don’t have a lot of data yet, there is a strong consensus that puberty blockers are helpful. A very large and recent study showed that transgender youth who want puberty blockers and are put on them are likely to see a reduced amount of lifetime suicidal ideation compared to those who want puberty blockers and are denied them (Turban et al., 2020). The American Academy of Pediatrics, taking account of what studies exist, observes that “pubertal suppression in children who identify as TGD [transgender or gender diverse] generally leads to improved psychological functioning in adolescence and young adulthood.” The upsides for youth who need them are massive financially as well, since transitioning is far more expensive after going through an unwanted puberty. This doesn’t mean that they are without risks; rather, it just means that these risks are generally justified. In particular, WPATH notes that suppressing puberty may cause issues with bone development and decrease height. However, the possible alternative is that “functioning in later life can be compromised by the development of irreversible secondary sex characteristics during puberty and by years spent experiencing intense gender dysphoria.” (See p. 20 of the WPATH link above.) If given a choice between somewhat weaker bones and crippling mental difficulties, I think most would choose the former.
For transfeminine youth, another relevant consideration is future genital reconstruction surgery (discussed further in the section on surgical interventions below). Puberty blockers followed by cross-sex hormones (discussed further in the section on cross-sex hormones below) may lead to the penis never growing further, meaning there won’t be enough material for penile inversion vaginoplasty, the most common type of vaginoplasty (surgical creation of a vagina). There are other forms of vaginoplasty that can be done if this is a problem.
Slightly more difficult is the question of fertility. If puberty suppression is promptly followed up with cross-sex hormones, then fertility may never develop. This is why, as far as I have seen, all professional organizations who have any level of detailed guidelines on this topic strongly recommend that the adolescent and their guardians be counseled on the fact that they may become infertile. Of course, saving fertility only for the adolescent to commit suicide is hardly a net gain, and many transgender adults consider giving up fertility for better mental and social health a fair trade, if they were ever even interested in having biological children.
Any other risks are minor or unknown. For example, some claim that puberty suppression followed up with cross-sex hormones leads to an inability to have any sexual satisfaction at all. This is pure myth, unsupported by reality. Two recent overviews of sexual health in transgender youth published in peer reviewed journals (T’Sjoen et al., 2020; Mehringer & Dowshen, 2019) make no mention of this being a problem. The long-term effects aren’t quite clear yet, but the existing data is strong enough that clinicians feel comfortable providing puberty blockers to adolescents. I’m inclined to believe that they are better able to weigh the risks than I am.
Cross-sex hormones
The general rule of thumb is that transgender adolescents are not given cross-sex hormones (CSH) until they are at least 16 years of age, and ideally with the support of their family. This also is reflected in the three sources I linked above. CSH are regarded as partially reversible because after a few months on them, most people begin to develop changes that do not go away if they cease taking them. For example, facial hair spurred on by testosterone therapy and breast growth induced by feminizing hormone therapy remain even if the hormone therapy is stopped. Because of this, these are more tightly restricted than puberty blockers, with a higher bar to meet before being prescribed them. Some clinicians consider the possibility of CSH prior to 16, but this is rare, and is typically scrutinized. The only reasonable justification for this is the presence of intense, crippling dysphoria accompanied by strong depression and/or anxiety which seems remediable through hormone therapy. Extreme suicidality or an inability to function whatsoever tends to justify risky responses, but this is rare. The vast majority of trans youth wait until at least 16 to receive hormone therapy.
As already mentioned, gender dysphoric adolescents are far more likely to identify as transgender into adulthood than dysphoric children. By the time that they are 16, assuming there are no complicating factors such as them being uncertain about their gender or confounding mental health issues, the likelihood that their identity is stable is fairly strong. This is reflected in a follow-up study of 70 adolescents who were diagnosed with gender dysphoria and given puberty blockers: All 70 stuck around to continue CSH (de Vries et al., 2010). Given the amount of children who are lost to follow-up or desist in studies on dysphoric children (see my article on desistance), this would be incredibly unlikely unless transgender adolescents are far more likely to persist than transgender children.
The risks of CSH are fairly well documented, and are justified as long as there are no any serious individual health problems. The most serious risks for feminizing hormone therapy are venous thromboembolism (blood clot in a vein deep in the leg), hypertriglyceridemia (high levels of fat in the blood), and, if there are preexisting risk factors, cardiovascular disease (problems with the heart and blood vessels), type 2 diabetes, and hypertension (high blood pressure). For masculinizing hormone therapy, the main risks are polycythemia (too many red blood cells causing the blood to thicken) and hyperlipidemia (high levels of fat in the blood). While this might sound scary, developing any of these is quite unlikely — and these are the most likely and serious side effects to get from hormone therapy. These risks can also be offset by things like exercise, diet changes, and taking the hormones a different way (for example, as a shot instead of pill). As with puberty blockers, these risks are typically quite small. Doctors ask questions to make sure the risks aren’t too high prior to prescribing CSH. (Much of this paragraph is taken from Appendix B of the WPATH SoC v7.)
Occasionally, a transgender adolescent will express that they do not want to look completely stereotypically feminine or masculine. In these cases, it is possible to use CSH for a limited time, so as to gain some of the irreversible effects, or at a lower dosage. This is a relatively new approach.
Surgical interventions
Genital reconstruction surgery (variously called sexual reassignment surgery, gender affirmation surgery, gender reassignment surgery, and genital reassignment surgery, among others) or a hysterectomy (removal of the uterus) is 100% not recommended for anyone below the age of 16, and that is only if 16 is the legal age of majority in their country. In addition to this, the standard is that these surgeries only be given if the transgender person has been living as their desired gender for a year (to ensure confidence, since surgical interventions aren’t really reversible!) and, unless there’s health concerns that make it unwise, at least a year on CSH. Surgery is a serious deal and it is well outside standard practice to do anything less than what I’ve outlined here, and many health practitioners would ask more prior to greenlighting it.
Chest masculinization is sometimes available earlier. WPATH suggests it only be done after a year on masculinizing hormone therapy and a year living as their desired gender, while acknowledging that there may be situations where it could be done sooner. The Endocrine Society notes that there is not enough evidence to suggest a specific age requirement, but advises clinicians to take into account the physical and mental health of the patient.
The bigger picture
So far, most of this article has been about medical interventions. That’s because most of the misinformation and panic revolves around them. However, that is an extremely narrow and insufficient view of transgender youth. Trans Kids and Teens by Elijah C. Nealy is over 300 pages long. Only about 30 of those pages — less than 10% — are devoted to medical interventions. The rest of the book discusses therapy, coming out, family relationships, managing school, and the transition into adulthood. Similarly, the nine page “Gender dysphoria in childhood” (Ristori & Steensma, 2016) spends virtually no time on medical treatment. In an op-ed written for the New York Times, Dr. Jack Turban, who specializes in LGBT youth and youth psychiatry, clearly explains that there is far more to transgender youth than medical interventions, and that the panic surrounding their treatment is liable to cause great harm. Among the dangers: Without professional help, dysphoric youth will seek relief in whatever way they can, even if it causes substantial bodily harm. Many transgender youth DIY, the risky practice of illegally obtaining hormones for self-medication, and it’s all-too-common for transmasculine youth bind their chest with the wrong materials, resulting in serious rib injuries.
To a lesser extent, there’s also some panic about transgender youth in sports and “social contagion.” As I’ve discussed previously, demanding strict sex-segregation in sports before the child is well into puberty makes absolutely no sense whatsoever. With regards to social contagion, there is an idea floating around that children only get gender dysphoria because they’ve heard about transgender people, and so all that is needed to prevent it is to keep children from ever hearing about it. Society previously tried this idea with homosexuality: Keep a kid from knowing about gay people, and they won’t be gay! It didn’t work out. As it turns out, depriving children of knowledge of “a common and culturally-diverse human phenomenon [that] should not be judged as inherently pathological or negative,” as the World Professional Association for Transgender Health puts it, is not conducive to their mental health. (I’ve previously discussed the single study that people use to support the idea of social contagion among transgender youth here.)
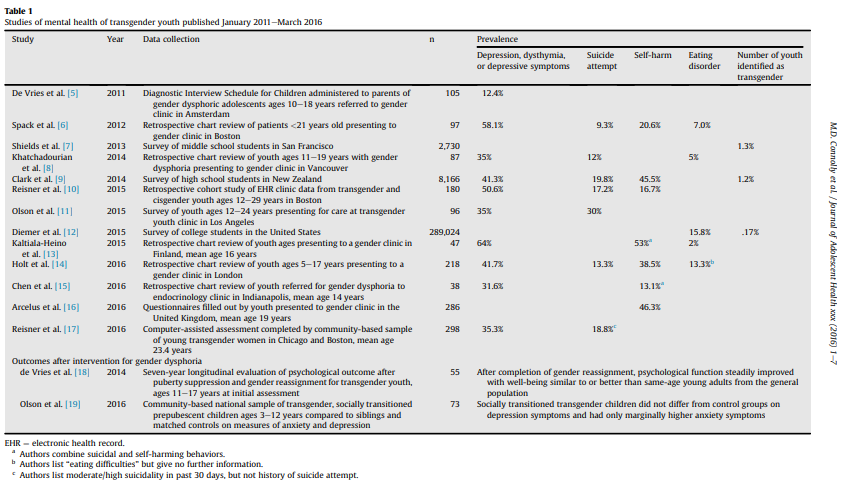
Let’s focus on reality. The reality is that being accepted by their family is something any child needs. Guardians will often have a hard time accepting or adapting to their child being transgender or gender-nonconforming, so group therapy is often very helpful. Given that transgender youth are frequently bullied and harassed, surrounding them with supportive peers is very important. Paperwork issues are often a huge hassle when someone is transgender, so transgender youth need help from their guardians, and they will in turn need help figuring out what to file. Since TGNC youth are far more likely than their cisgender peers to have depression or anxiety, if not other coexisting mental health problems (Connolly et al., 2016), it’s extremely important to pay close attention to their functioning and risk for self-harm and suicide. Coming of age is hard for everyone, but is doubly so for TGNC adolescents; they will need extra support there.
This topic is salient for a lot of transgender people because we remember what it was like to be a kid in the closet. According to the 2015 United States Transgender Survey, over half of the respondents began to feel “different” than other people by age 10, and over half began to think they were transgender by age 15. Many of us were bullied for not acting “right” by society’s norms. Many of us hid from our parents, or were hurt by our parents, or kicked out of our homes. And the vast majority of us had to deal with our bodies changing in ways that we really, really didn’t want them to. The next generation of transgender people might not have to go through what we did.
As far as I can tell, a majority of the literature on TGNC youth is psychological in nature, not hormonal or surgical. The conversation should reflect this, not just to keep itself tethered to evidence, but to reflect the very real lives that they live. They’re not the latest fad or your new wedge issue. They’re children, for Christ’s sake.
References
Coleman, E., Bockting, W., Botzer, M., Cohen-Kettenis, P., DeCuypere, G., Feldman, J., Fraser, L., Green, J., Knudson, G., Meyer, W.J., & Monstrey, S. (2012). Standards of care for the health of transsexual, transgender, and gender-nonconforming people, version 7. International journal of transgenderism, 13(4), 165-232. Retrieved from https://www.wpath.org/media/cms/Documents/SOC%20v7/Standards%20of%20Care%20V7%20-%202011%20WPATH.pdf?_t=1605186324 (PDF)
Connolly, M. D., Zervos, M. J., Barone II, C. J., Johnson, C. C., & Joseph, C. L. (2016). The mental health of transgender youth: Advances in understanding. Journal of Adolescent Health, 59(5), 489-495.
De Vries, A. L., Steensma, T. D., Doreleijers, T. A., & Cohen‐Kettenis, P. T. (2011). Puberty suppression in adolescents with gender identity disorder: A prospective follow‐up study. The Journal of Sexual Medicine, 8(8), 2276-2283.
Hastings, J. (2016, June 17). Approach to genderqueer, gender non-conforming, and gender nonbinary people. UCSF Transgender Care. Retrieved from https://transcare.ucsf.edu/guidelines/gender-nonconforming
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. (2017, September 1). Gender Dysphoria/Gender Incongruence Guideline Resources. The Endocrine Society. Retrieved from https://www.endocrine.org/clinical-practice-guidelines/gender-dysphoria-gender-incongruence
James, S., Herman, J., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. A. (2016). The report of the 2015 US transgender survey.
Mehringer, J., & Dowshen, N. L. (2019). Sexual and reproductive health considerations among transgender and gender-expansive youth. Current Problems in Pediatric and Adolescent Health Care, 49(9), 100684.
Nealy, E. C. (2017). Trans Kids and Teens: Pride, Joy, and Families in Transition. WW Norton & Company.
Rafferty, J., & Committee on Psychosocial Aspects of Child and Family Health. (2018). Ensuring comprehensive care and support for transgender and gender-diverse children and adolescents. Pediatrics, 142(4).
Ristori, J., & Steensma, T. D. (2016). Gender dysphoria in childhood. International Review of Psychiatry, 28(1), 13-20.
T'Sjoen, G., Arcelus, J., De Vries, A. L., Fisher, A. D., Nieder, T. O., Özer, M., & Motmans, J. (2020). European Society for Sexual Medicine position statement “Assessment and hormonal management in adolescent and adult trans people, with attention for sexual function and satisfaction”. The Journal of Sexual Medicine.
Turban, J. L. (2020, February 6). What South Dakota Doesn’t Get About Transgender Children. New York Times. Retrieved from https://www.nytimes.com/2020/02/06/opinion/transgender-children-medical-bills.html
Turban, J. L., King, D., Carswell, J. M., & Keuroghlian, A. S. (2020). Pubertal suppression for transgender youth and risk of suicidal ideation. Pediatrics, 145(2).